Chronic Superficial Keratitis, CSK (Pannus) – Canine
Rachel L. Davis1
VIN Publication
Abstract
Glaucoma refers to elevated intraocular pressure (IOP) that is either sustained or fluctuating. It can ultimately result in death of retinal ganglion cells. Glaucoma encompasses a broad category of diseases but is commonly referred to in the singular tense. Although normotensive glaucoma has been identified in people, it has not been documented in the cat or dog.
Chronic superficial keratitis (pannus) is an immune-mediated corneal disease in dogs, especially German shepherds, causing pigmentation and vascularization. Learn about causes, clinical signs, diagnosis, treatment, and long-term management below.
Keywords: chronic superficial keratitis in dogs, pannus in dogs, canine pannus eye disease, plasmoma of the third eyelid in dogs, immune mediated corneal disease in dogs, german shepherd pannus, breeds predisposed to pannus, causes of pannus in dogs, diagnosis of pannus in dogs, treatment of pannus in dogs, cyclosporine implants for pannus, UV light exposure and pannus, topical therapy for canine pannus, subconjunctival steroid pannus treatment, pannus disease management in dogs, prognosis for pannus in dogs, plasmacytic conjunctivitis third eyelid, pannus vs pigmentary keratitis, pannus seasonal flare-ups in dogs
Contributors:
1Revised by Rachel Davis DVM, MS, DACVO at Animal Eye Clinic, Westfield, Indiana, USA, on 5/13/2021
Original author was Ian P. Herring DVM, MS, DACVO, 1/25/2004
Correspondence:
Rachel L. Davis, DVM, MS, Diplomate, ACVO – Ophthalmologist
Animal Eye Clinic
4750 Killarney Drive
Carmel, IN 46033
Email: info@indyaec.com
Synonyms:
Pannus
Uberreiter’s syndrome
Plasmoma of third eyelid
Plasmacytoma of the third eyelid
Disease Description:
Definition
Chronic superficial keratitis (CSK) or pannus, is a bilateral disorder of the canine cornea characterized by progressive, often raised, corneal vascularization, hazy opacification (white or grayish) and pigmentation.1 In approximately 70% of cases, the third eyelid is concurrently affected (i.e. plasmoma/plasmacytoma/plasmacytic conjunctivitis).2
Etiology
Pannus is likely an immune-mediated condition as recent evidence suggests an altered haplotype3 of major histocompatibility (MHC) class II or abnormal MHC class II expression4 as contributory in disease development. CD4-expressing lymphocytes are the predominant infiltrative cell type in CSK.5 The German shepherd dog (GSD) has a strong breed predilection, which suggests pannus may also be heritable.2,6,7 This is further supported by a study examining genetic upstream regulatory regions in GSDs which revealed that GSDs homozygous at DRB1*69 [C/T] had four times the risk of developing CSK compared to heterozygotes.19
Increased UV light exposure also mediates development of CSK, with altitude significantly affecting the prevalence of the disease.8 UV light increases expression of corneal matrix metalloproteinase-2 (MMP-2), an inflammatory mediator that is also increased in corneal cells from CSK patients, suggesting a link to UV light-induced MMP-2 upregulation with disease development.9
Diagnosis
Ophthalmic Examination Findings: Diagnosis can usually be made based on the appearance of the corneal lesions in breeds typically affected by the disease. The lesions are not painful and are comprised of small to large areas of red, brown or gray discoloration in the cornea (Figure 1). The third eyelid margin may have concurrent depigmented, thickened, irregular hyperemic lesions (Figure 2). Corneal lesions typically arise at the ventral-nasal, ventral-temporal or temporal limbus. Lipid deposits may develop along the leading edge (Figure 3). Fluorescein staining is negative; however, fluorescein may “stipple” or pool in areas of raised, irregular cornea. Because other conditions may cause similar corneal changes, a thorough examination assessing quantitative tear production, adnexal surfaces and fluorescein staining is warranted.
Cytology: Cytology of conjunctival scrapings reveals lymphoplasmacytic inflammation. This is not typically necessary for diagnosis due to the characteristic appearance of the lesions after other causes of corneal granulation and pigmentation are ruled out.
Disease Description in This Species:
Signalment
Although the GSD and GSD-cross dogs are affected most often, CSK has also been reported in the Australian shepherd, Belgian tervuren, Belgian shepherd, border collie, greyhound, rottweiler, Rhodesian ridgeback, and Siberian husky.4,7,20,21 It can occur sporadically in other purebred or mixed breed dogs.
Some studies report a higher prevalence in male dogs2,8 while another study reported a higher incidence in female dogs.3 A true sex predisposition for the disease is unlikely. Dogs are most often affected between 5-8 years of age.2
Clinical Signs
Most dogs are presented because of a change in the appearance of their eyes. The condition is not painful but can be accompanied by mucoid to mucopurulent discharge. Lesions typically arise from the ventral-nasal or ventral-temporal or temporal limbus (Figure 1), although it may occur anywhere along the limbus and cornea. The lesions are comprised of small to large areas of red, brown or gray discoloration in the cornea that are followed by superficial pigment (Figure 1). Lipid deposits may develop along the leading edge (Figure 3). If the disease is not treated, it may progress to involve large areas of the cornea, which may affect vision (Figure 1).
When the third eyelid is affected, lesions typically appear as hyperemic, irregular, variably depigmented areas visible along the anterior conjunctival surface (Figure 2).2 Third eyelid involvement may occur concurrent with or independently of corneal lesions (Figure 2).
Etiology:
Genetic, hereditary
Idiopathic, unknown
Immune-mediated disease
Ultraviolet light
Breed / Species Predilection:
Australian shepherd
Belgian shepherd
Belgian tervuren
Border collie
German shepherd cross
German shepherd dog
Greyhound
Large breed dogs
Siberian husky
Sex Predilection:
None
Age Predilection:
Mature, middle-aged
| Diagnostic Procedures: | Diagnostic Results: | |
| Cytology, biopsy of conjunctiva or cornea | Lymphoplasmacytic cellular infiltration |
Images:
Figure 1: Chronic superficial keratitis presentation.
Typical CSK lesions include temporal to ventral raised, irregular corneal vascularization with admixed pigment and fibrosis. The lesions can be perilimbal (1a) or can extend to the central cornea (1b) and even affect the cornea diffusely in severe cases (1c).
Figure 2: Plasmacytoma of the third eyelid
The third eyelid may or may not be affected in cases of CSK. When present, plasmacytoma appears as raised, depigmented conjunctival granulation as depicted in this middle-aged GSD (Figure 2a). Plasmacytoma may also be present independent of corneal lesions as shown in this 6yr old Rhodesian ridgeback (Figure 2b). After treatment, the third eyelid returned to normal in both cases (Figure 2c).
Figure 3: Lipid deposition at leading edge of CSK lesions.
Lipid may be variably present at the leading edge of CSK lesions. The lipid may appear as multifocal white stromal opacities (Figure 3a) or may present as a larger, focal region of lipid. Lipid opacifications may be persistent, even after control of the active corneal disease (Figure 3b and 3c).
Figure 4: Topical treatment for CSK and plasmacytoma.
This middle-aged GSD has CSK that has been controlled for over three years with ongoing topical therapy. On initial presentation, there was significant corneal opacification and third eyelid granulation (Figure 4a). Three years after diagnosis, the cornea has minimal opacification and mild lipidosis while the third eyelid remains normal (Figure 4b).
Figure 5-7: Cyclosporine implantation and subconjunctival steroid administration for CSK.
Three GSD’s were treated for CSK using cyclosporine implant placement as well as initial or infrequently repeated subconjunctival steroid injections. The implants are replaced every 8-12 months to control the condition long term. Figure 5a, 6a and 7a are photographs at diagnosis while Figure 5b, 6b and 7b demonstrate the eyes after treatment.
Figure 8: UV protective eyewear as supplemental therapy for CSK.
A young Labrador retriever is depicted wearing a type of protective eyewear. These goggles (or ones that have two eyepieces) are generally well-tolerated after positive-reinforcement training.
Figure 9: Residual corneal pigmentation in patients with CSK.
As depicted in these photographs, some corneal pigmentation may be permanent, even after control of CSK lesions. Figure 9a depicts a middle-aged GSD two years after initial diagnosis of CSK. This patient is maintained with cyclosporine implantation every ten months. Figure 9b represents a young mixed breed dog three years after CSK diagnosis maintained on topical therapy. For reference, the patient in 9a is pictured at initial diagnosis in Figure 9c and the patient in 9b is pictured at initial diagnosis in Figure 9d. As long as the pigment is not progressive over time or interfering with vision, it is not overly concerning.

Figure 1A. Pannus OD.
Click here to see board discussion
Figure 1B. Pannus OS.
Click here to see board discussion
Figure 2. Pannus – Rhodesian ridgeback.
Click here to see board discussion
Figure 3. Chronic superficial keratitis in a 6-year-old German shepherd. Corneal vascularization and pigmentation originating at the temporal limbus and progressing centrally is evident. Note the faint corneal lipid infiltrates central to the leading edge of the vascularization. 
Figure 4A. Infiltrative pigment associated with CSK. The pigment originates from the temporal limbus and is admixed with arborizing corneal vessels present. 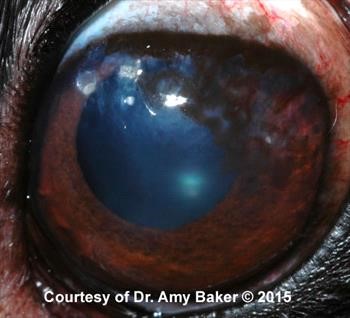
Figure 4B. CSK patient after 4 wks of topical therapy. Note multifocal thinning of pigment. Now the iris is visible through the pigment in some areas. 
Figure 5. Pannus & lipid infiltrates in the cornea.
Click here to see board discussion
Figure 6. Severe pannus.
Click here to see board discussion
Figure 7. Plasmoma third eyelid.
Click here to see board discussion
Figure 8. Pannus & plasmoma third eyelid
URL: https://beta.vin.com/doc/?id=7421011
Treatment / Management:
SPECIFIC THERAPY
Topical therapy is the most common form of therapy for the majority of CSK cases. Topical cyclosporine,10,11 dexamethasone,10 tacrolimus in DMSO,12 and pimecrolimus13 have all been shown to significantly improve corneal lesions and plasmacytic conjunctivitis of the third eyelid. Typically, a combination of topical steroids (e.g. prednisolone acetate, dexamethasone) and immune-modulating therapy (e.g. tacrolimus, cyclosporine) are administered initially, depending upon the severity of the lesions. Mild lesions may be responsive to topical steroids alone; however, these medications may cause other corneal disease long term. Therefore, topical immune-modulating therapy is ideal for long term use. Frequency of administration ranges from q 6-12 hrs initially until the disease is controlled. The disease is considered controlled once all vascularization and raised areas have receded from the cornea and all lesions of the third eyelid have resolved (Figure 4). Frequency is then tapered to the lowest effective dose for long term control.1 Treatment must be administered long term for disease control.
Subconjunctival steroids may be considered for severe cases with decreased vision, eyes that are refractory to topical therapy, or preliminary therapy for patients initially resistant to topical medication instillation. Ophthalmic betamethasone 1-2 mg or triamcinolone 4 mg may be injected subconjunctivally (Figure 5). The injections may be repeated at intervals of 6-12 months as needed to control the disease in conjunction with cyclosporine or tacrolimus therapy.
Subconjunctival cyclosporine implantation
Recently, subconjunctival cyclosporine implantation has been used to treat CSK[RD1] (Figures 5-7). Referral to a veterinary ophthalmologist for implantation may be considered for patients that will not tolerate topical therapy or for clients that prefer not to instill daily topical eye medication.
Other therapies for refractive cases include radiotherapy using soft X-rays,14 strontium-90 therapy (with or without superficial keratectomy),15 and cryotherapy16. These therapies have been partially successful when used concurrently with aggressive topical therapy but recurrence is likely over time.
SUPPORTIVE THERAPY
Because CSK is worsened by UV light, decreased exposure to UV light is recommended for dogs with this disease. UV-blocking contact lenses have not been shown to be helpful as an adjunctive therapy for dogs with CSK, although secondary corneal irritation from prolonged contact lens wear likely affected the results.17 In addition to topical therapy, it may be helpful to keep affected dogs inside during the day; provide them with shelter out of the sun; or consider the use of UV protective eyewear during outdoor activity (Figure 8). Studies are lacking on the effects of UV protective eye wear but anecdotally these goggles seem to be beneficial for dogs that spend extended periods of time outside (e.g. working and military dogs, dogs hiking in mountainous regions, etc.).
MONITORING and PROGNOSIS
Long-term topical therapy is required to control CSK because it typically recurs with discontinuation of therapy. Rechecks may be done within 3-4 weeks of instituting therapy. After this, re-evaluation is performed periodically as the lowest effective dose is attained based on patient response. Once the disease is controlled, re-evaluation may be done q 4-6 months.
Middle-aged to older dogs and dogs living in areas of lower UV light levels (e.g. lower altitudes) typically respond well to topical therapy and may be managed long term with topical therapy alone.1 Seasonal worsening of the disease during the summer (i.e. “flare-up”) is common. Corneal pigment may improve within weeks of starting therapy or may take several months to improve. Some permanent, residual corneal pigment is common (Figure 9). Lipid infiltrates are also usually permanent but may decrease with time, especially if topical steroids are discontinued after the initial treatment phase (Figure 3).
Special Considerations:
Other Resources:
Recent VIN Message Board discussions on chronic superficial keratitis
VIN Message Board discussions on plasmoma of third eyelid
Client handout on pannus
Proceedings articles that discuss CSK
For more images of corneal lesions see the Pannus, Part 1 – Dog slideshow in the Image Library
For more images of corneal lesions see the Pannus, Part 2 – Dog slideshow in the Image Library
For more images of third eyelid lesions see the Plasmoma Third Eyelid slideshow in the Image Library
Differential Diagnosis:
Because corneal pigmentation, vascularization and opacification may occur with chronic corneal irritation associated with keratoconjunctivitis sicca, trichiasis, distichiasis or ectopic cilia, these abnormalities must be ruled out. Pannus is not painful, which helps to differentiate it from other causes of corneal pigmentation and vascularization.
Corneal granulation tissue
Keratoconjunctivitis sicca
Pigmentary keratitis/keratopathy
Squamous cell carcinoma of cornea or third eyelid: rare, unilateral
References:
- Gilger B C, Gelatt KN : Diseases and Surgery of the Canine Cornea and Sclera. Veterinary Ophthalmology , 4th ed. Blackwell Publishing, Oxford UK pp. 722-23.
- Drahovska Z, Balicki I, Trbolová A, et al: A retrospective study of the occurrence of chronic superficial keratitis in 308 German Shepherd dogs: 1999-2010. . Pol J Vet Sci 2014 Vol 17 (3) pp. 543-6.
- Jokinen P, Rusanen E M, Kennedy L J et al: MHC class II risk haplotype associated with canine chronic superficial keratitis in German Shepherd dogs.. Vet Immunol Immunopathol 2011 Vol 140 (1-2) pp. 37-41.
- Williams D L : Major histocompatibility class II expression in the normal canine cornea and in canine chronic superficial keratitis . Vet Ophthalmol 2005 Vol 8 (6) pp. 395-400.
- Williams D L: Histological and immunohistochemical evaluation of canine chronic superficial keratitis. Res Vet Sci 1999 Vol 67 (2) pp. 191-5.
- Stanley R G: Superficial stromal keratitis in the dog. Aust Vet J. 1988 Vol 65 (10) pp. 321-3.
- Bedford P G, Longstaffe J A: Corneal pannus (chronic superficial keratitis) in the German shepherd dog. J Small Anim Pract 1979 Vol 20 (1) pp. 41-56.
- Chavkin MJ, Roberts SM, Salman MD, et al: Risk factors for development of chronic superficial keratitis in dogs. J Am Vet Med Assoc 1994 Vol 204 (10) pp. 1630-1634.
- Chandler H L, Kusewitt D F, Colitz C M H: Modulation of matrix metalloproteinases by ultraviolet radiation in the canine cornea. Vet Ophthalmol 2008 Vol 11 (3) pp. 135-44.
- Williams D L, Hoey A J, Smitherman P: Comparison of topical cyclosporin and dexamethasone for the treatment of chronic superficial keratitis in dogs. Vet Rec 1995 Vol 137 (25) pp. 635-9.
- Read RA: Treatment of canine nictitans plasmacytic conjunctivitis with 0.2 per cent cyclosporin ointment. J Small Anim Pract 1995 Vol 36 (2) pp. 50-6.
- Balicki I: Clinical study on the application of tacrolimus and DMSO in the treatment of chronic superficial keratitis in dogs. Pol J Vet Sci 2012 Vol 15 (4) pp. 667-76.
- Nell B, Walde I, Billich A, et al: The effect of topical pimecrolimus on keratoconjunctivitis sicca and chronic superficial keratitis in dogs: results from an exploratory study. Vet Ophthalmol 2005 Vol 8 (1) pp. 39-46.
- Allgoewer I, Hoecht S: Radiotherapy for canine chronic superficial keratitis using soft X-rays (15 kV). . Vet Ophthalmol 2010 Vol 13 (1) pp. 20-5.
- Höcht S, Grüning G, Allgoewer I, et al: [Treatment of keratitis superficialis chronica of the dog with strontium 90] . Strahlenther Onkol 2002 Vol 178 (2) pp. 99-104.
- Azoulay T: Adjunctive cryotherapy for pigmentary keratitis in dogs: a study of 16 corneas. Vet Ophthalmol 2014 Vol 17 (4) pp. 214-9.
- Denk N, Fritsche J, Reese S, et al : The effect of UV-blocking contact lenses as a therapy for canine chronic superficial keratitis. Vet Ophthalmol 2011 Vol 14 (3) pp. 186-98.
- Balicki I, Sobczyńska-Rak A: Serum vascular endothelial growth factor concentration in dogs diagnosed with chronic superficial keratitis. Acta Vet Hung 2014 Vol 62 (1) pp. 22-23.
- Barrientos L S, Zapata G, Crespi J A, et al: A study of the association between chronic superficial keratitis and polymorphisms in the upstream regulatory regions of DLA-DRB1, DLA-DQB1 and DLA-DQA1. . Vet Immunol Immunopathol 2013 Vol 156 (3-4) pp. 205-10.
- Gionfriddo J R, Powell C: A Greyhound With Red Eyes. Vet Med, 8 Refs ed. 2005 Vol 100 (4) pp. 264-68.
- Vet Ophthalmol: Ophthalmic examination findings in a group of retired racing Greyhounds . Lynch G L 2007 Vol 10 (6) pp. 363-37.